
Jaw bone atrophy


What is jawbone atrophy?
Bone tissue atrophy is a pathology manifested by a reduction in the jawbone. The first signs of loss can appear as early as 2.5-3 weeks after tooth loss.
Chewing pressure is not distributed to the area without a tooth. Nutrients and building cells in the jaw structure become less. Tissues atrophy, and the gums thin. Over time, the process worsens. The longer the jaw section remains unloaded, the greater the loss and the more difficult it is to restore the original volumes.
How does bone loss occur?
The absence of chewing pressure on toothless areas reduces the efficiency of osteoblasts, which are responsible for bone construction. Therefore, new cells appear slowly, while the destruction of old ones accelerates. New cells do not have time to replenish volumes - bone loss occurs.
Structure of bone tissue
The jaw volume consists of two layers that are uneven in structure:
- Cortical plate – the upper dense layer of the jaw. It contains many formed bone cells (osteocytes). But there are few osteoblasts - young cells that eventually turn into osteocytes. The more osteocytes in the cortical layer, the slower the atrophy occurs. However, a pronounced, dense cortical plate creates difficulties in implantation and volume restoration of the jaw
- Spongy bone – the inner layer with actively dividing young cells. Mature bone structures are significantly fewer here, so the spongy layer is less durable, prone to atrophy, but better amenable to restoration.
Different people have different ratios of spongy layer and cortical plate. Therefore, implantologists use the classification of bone tissue biotypes:
- D1
- thick cortical plate with almost no spongy substance;
- D2
- thick cortical layer surrounded by a thin spongy substance;
- D3
- a small amount of cortical bone surrounded by a large amount of spongy substance;
- D4
- a large fragile spongy layer with a thin cortical plate.
Biotype – a local measure that can vary in different parts of the jaw. Knowing the biotype in the area of surgical intervention in advance can help predict the degree of resorption even before tooth extraction. This helps the implantologist plan the operation correctly.
When does bone tissue atrophy begin?
Each person experiences resorption differently. For example, in people with biotype D4, the loss can start 2-3 weeks after tooth extraction, but restoring volumes is easier because the structure is looser. In patients with biotype D1, resorption may not appear for years, but it is much more difficult to restore.
In youth, atrophy progresses more slowly than in people after 40-50 years.
What causes jawbone atrophy?
- Tooth extraction/absence. The toothless area of the jaw stops being functionally loaded, leading to narrowing of blood vessels and slower renewal of cellular structures. The loss of the alveolar part begins as early as 2.5-3 weeks and reaches a maximum within a year.
- Chronic inflammatory process. Inflammation in the jaw tissue disrupts the work of bone cells, slowing the formation of new structures. The process occurs with periodontitis, periodontal disease, root cysts, etc.
- Mechanical trauma. Jaw fractures, alveolar process contusions can trigger resorption processes.
- Osteoporosis. A pathological condition in which microelements are washed out of the bone. Thus, its density decreases, and resorption processes are triggered. Osteoporosis can be an independent disease or occur against the background of endocrine pathologies, chronic inflammatory diseases of the gastrointestinal tract, reproductive system dysfunctions, etc.
Degrees of jawbone atrophy
-
Mild
Resorption is minimal. Volume restoration is not required, but orthopedic treatment is necessary for prevention.
-
Moderate
Resorption is more pronounced. Poor fixation of orthopedic constructions. It is impossible to install implants without preliminary restoration of bone level.
-
Severe
Severe resorption. Prosthetics are impossible without preliminary osteoplasty.
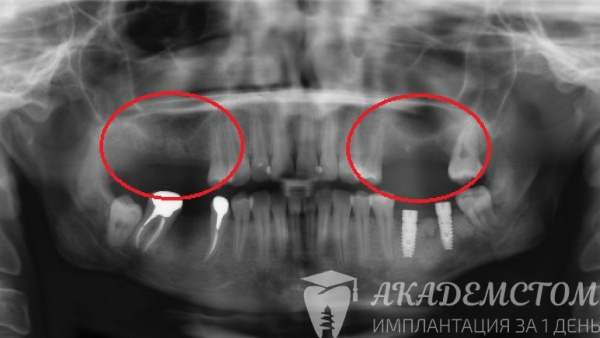
How is the degree of loss diagnosed?
To detect jaw resorption, implantologists use:
- Oral cavity examination. The doctor notes the patient's facial proportions, examines the tooth rows, assesses the structure and density of the alveolar part of the jaw in places where teeth are missing.
- 3D dental scan (CBCT). A modern study that allows evaluating structures in three-dimensional space, as well as seeing all anatomical formations located close to the surgical field.
In the Kiadent clinic, performing a CT scan is a mandatory condition when planning implantation. CT quickly allows assessing the condition of the bone, seeing the distance to important anatomical formations, and finding the optimal position for the implant.
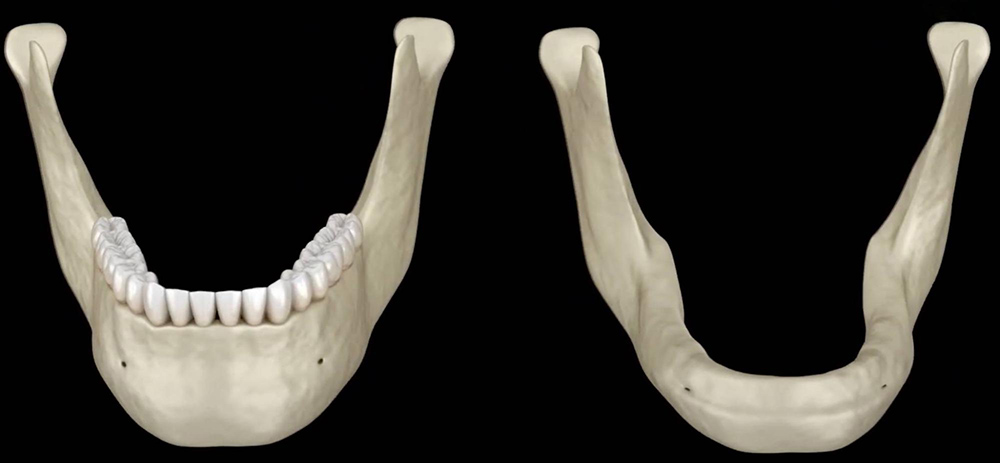
Features of lower jawbone atrophy
The lower jaw is a movable structure involved in chewing. This is where the main chewing load falls. The alveolar ridge is loose, so resorption occurs faster. Installing implants on the lower jaw is faster and easier than on the upper jaw because the tissues are not very dense. Moreover, the grafted bone material here takes root faster.
Doctor's opinion:
In cases where there is not enough tissue for implantation, there is a risk of nerve damage. This can lead to numbness of the lips, cheeks, tongue, and skin areas. Sensitivity recovery takes up to 6-8 months, and sometimes it does not occur at all.
Features of upper jawbone atrophy
The upper jaw tissue is immovable – less subject to chewing loads, therefore less dense. The alveolar process diminishes faster. In some cases, even immediately after tooth extraction on the upper jaw, osteoplasty is required.
Doctor's opinion:
Implantation on the upper jaw may be impossible due to the proximity of the maxillary sinuses. If there is little volume, there is a risk of the implant entering the sinus. This complication can provoke chronic sinusitis.
How is implantation performed in the case of bone tissue atrophy?
If there is not enough bone volume for implantation, the specialist will restore tissue loss using one of the methods before the operation.
Alveolar ridge splitting
It is performed when there is insufficient tissue width. Bone material is added inside the process, and when it grows with blood vessels, accelerated bone formation occurs.
After anesthesia, the doctor makes an incision in the mucous membrane, periosteum, and cortical plate, then uses special tools to expand the space and place the bone graft material.
On average, ridge restoration after splitting occurs within 3-4 months.
Guided bone regeneration
The operation involves restoring resorption with artificial materials. After the intervention, a strong framework of blood vessels and bone cells forms around the implant.
A bone graft is added to the surgical field, and a membrane is placed on top. The wound is sutured.
Material integration occurs within 3-4 months.
Sinus lift
Creating bone volume in the maxillary sinus area. The operation is indicated for restoring bone levels in the molar area of the upper jaw.
Depending on the initial tissue levels, the operation can be performed using one of two methods:
Closed sinus lift – performed when the initial volumes are more than 7 mm. Through a small hole in the gum, the doctor adds bone graft materials and covers them with a membrane. The closed sinus lift is less traumatic.
Open sinus lift needs to be performed when resorption is significant. The doctor lifts the gum and periosteum flaps, drills a hole in the bone, and opens access to the sinus. Carefully lifts the sinus wall and adds the material.
Bone block grafting
Own bone material in the wisdom teeth area of the lower jaw is grafted into the zone where there is bone tissue loss. The material is fixed with special small screws.
Can implantation be performed immediately after grafting?
Only after restoring the volumes can implantation be performed. In some cases, you will have to wait 4-6 months for the implants to be placed.
Zygomatic implantation in case of critical upper jawbone atrophy
In the case of severe bone tissue volume deficiency of the upper jaw, performing classic implantation or All-on-4 / All-on-6 is impossible without large-scale, complex osteoplasty. This is expensive (the operation costs 200-300 thousand hryvnias), traumatic (serious surgical operation), and long (rehabilitation lasts from 6 months to a year and a half).
In the Kiadent clinic, patients with pronounced bone loss restore all teeth within 3-7 days without bone grafting and sinus lift using zygomatic implantation. The zygomatic bone is used, not the jawbone. It is not prone to atrophy. Special elongated Zygoma or Zygomatic implants are used.
Performing zygomatic implantation according to the Zygoma protocol requires special knowledge in maxillofacial surgery and special training. Therefore, it is carried out only in some dental clinics in Odesa.
Koveshnikov Ihor Oleksiyovych (chief doctor of the "Kiadent" clinic) is a certified specialist in zygomatic implantation. He practices operations for installing zygomatic implants.
Prosthetics of the upper jaw on zygomatic implants Zygoma / Zygomatic have almost no contraindications. Implant survival is 99%. The rehabilitation period is short, the operation is non-traumatic.
Methods of treating jawbone atrophy
To restore volume, synthetic or natural materials are used. Natural transplants (autotransplants) are taken from the area where there is a lot of tissue and grafted into the resorption zone.
Synthetic materials (biomaterials) are foreign substances introduced into the body to perform certain functions.
Materials used to treat atrophy include:
- Osteograft
- “Bone substitute” that maintains space for the growth of new structures. The material does not resorb but gradually integrates into the host tissue.
- Mucograft
- “Gum substitute” designed to close mucous membrane defects. Mucograft serves as a framework for retaining migrating gum structures.
- Barrier membrane
- Collagen layer that separates tissues with different recovery rates. Bone regenerates slower, while the mucosa regenerates faster to prevent gums from growing into the space intended for bone tissue.
Questions and answers
- How quickly does bone tissue resorption begin after tooth extraction?
Each person experiences resorption at different speeds. It depends on the bone biotype, age, and overall health. On average, atrophy can start as early as 3 weeks after tooth loss.
- How can jawbone atrophy be prevented?
Timely treatment of carious lesions, restoration of damaged teeth, and prosthetics in the absence of teeth will help prevent bone volume loss.
- Does implantation stop bone atrophy?
Yes, tissue loss stops due to the activation of metabolic processes within the bone. Implantation replenishes the missing teeth, promoting proper distribution of chewing pressure across all jaw areas.
- Can bone tissue be increased by taking calcium?
With bone loss, taking calcium will be ineffective, as the source of bone formation is living cells, and microelements play a secondary role. The only effective way to increase bone is surgical intervention.




Koveshnikov Ihor Oleksiyovych
Horizontal and vertical atrophy are distinguished. Horizontal loss – insufficient bone width of the jaw, vertical – insufficient bone height. These types can combine with long-term tooth absence or extensive inflammation.